Dengue fever remains a serious public health threat in Malaysia, particularly during the monsoon season. According to the latest Clinical Practice Guidelines (CPG) for the Management of Dengue Infection in Adults (Malaysia), updated strategies have been implemented to ensure more accurate, effective, and life-saving treatment. This article provides a comprehensive overview of dengue management in Malaysia, based on the current CPG, including diagnosis, treatment, and prevention.
Epidemiology
Dengue is a major arthropod-borne viral disease with high morbidity and mortality, especially in tropical and subtropical urban areas. In Malaysia, dengue incidence has significantly increased—from 32 cases per 100,000 people in 2000 to 361 cases in 2014. Most cases (70–80%) occur in urban areas and affect those aged 15 and above.
Despite the rising incidence, Malaysia has managed to reduce the case fatality rate from 0.6% in 2000 to 0.2% in 2014, aligning with the national target. However, most dengue-related deaths still occur in those aged 15 and above, with the highest number recorded in 2004.
Dengue Virus And Serotype Trends In Malaysia
Dengue virus (DENV) is a mosquito-borne flavivirus transmitted by Aedes aegypti and Aedes albopictus, with four distinct serotypes: DENV-1, DENV-2, DENV-3, and DENV-4. Infection provides lifelong immunity to the same serotype but only temporary protection against others. Secondary infections increase the risk of severe dengue, due to antibody-dependent enhancement and other factors such as viral virulence, host genetics, T-cell response, viral load, and autoantibodies.
In Malaysia, all four serotypes co-circulate, but one serotype often predominates for about two years before being replaced. Notably, in 2014, the dominant serotype shifted twice from DENV-2 to DENV-1 between February and June.
Spectrum Of Dengue Infection
The incubation period for dengue infection is 4-7 days (range 3-14). It may be asymptomatic or may result in a spectrum of illness ranging from undifferentiated mild febrile illness to severe disease, with or without plasma leakage and organ impairment.
Symptomatic dengue infection is a systemic and dynamic disease with clinical, haematological and serological profiles changing from day to day. These changes accelerate within hours or even minutes during the critical phase, particularly in those with plasma leakage.
Course of Dengue Progression
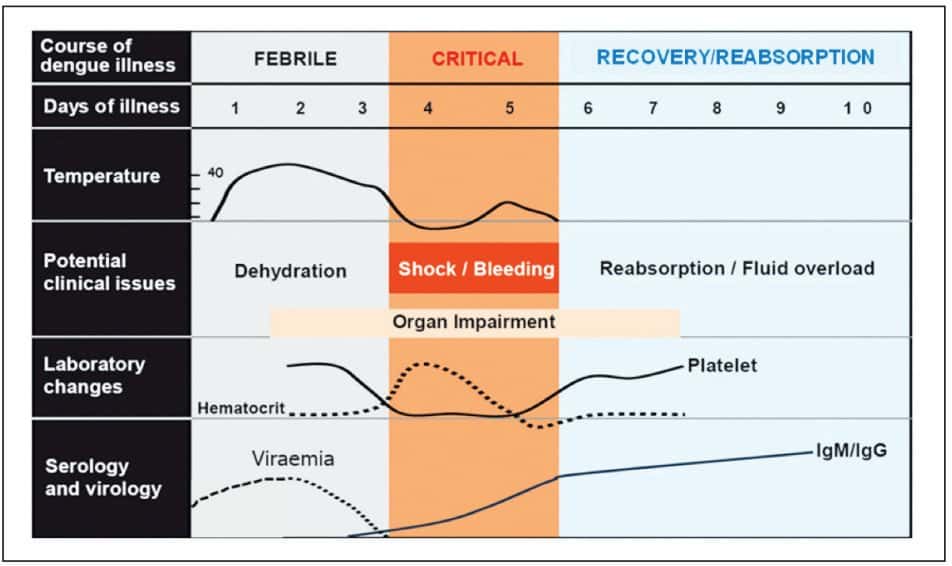
i. Febrile Phase
- Sudden high grade fever usually last 2-7 days.
- + facial flushing, rash, generalised body ache, vomiting and headache.
- +/- sore throat, injected pharynx and conjunctival injection.
- The findings of tender liver are warning signs of dengue infection.
- FBC -> progressive decrease in total white cell count followed by platelet reduction.
Bleeding
- Mild haemorrhagic manifestations like petechiae and mucosal membrane bleeding may be seen.
- Per vaginal bleeding may occur in females but rarely massive.
- Gastrointestinal bleeding is not uncommon.
ii. Critical Phase
Occurs after third day of fever (or earlier) or around defervescence(rapid drop in temperature) and lasts about 24-48 hours . This coincides with an increase in capillary permeability in some patients.
In other viral infections, the patient’s condition improves as the temperature subsides, but the contrary happens in severe dengue infection wherein the patient may deteriorate and manifest third space plasma leakage or organ dysfunction
Many of these patients either recover spontaneously or after a short period of fluid or electrolyte therapy. In more severe forms of plasma leakage, the patients may develop compensated or decompensated shock (Table 1).
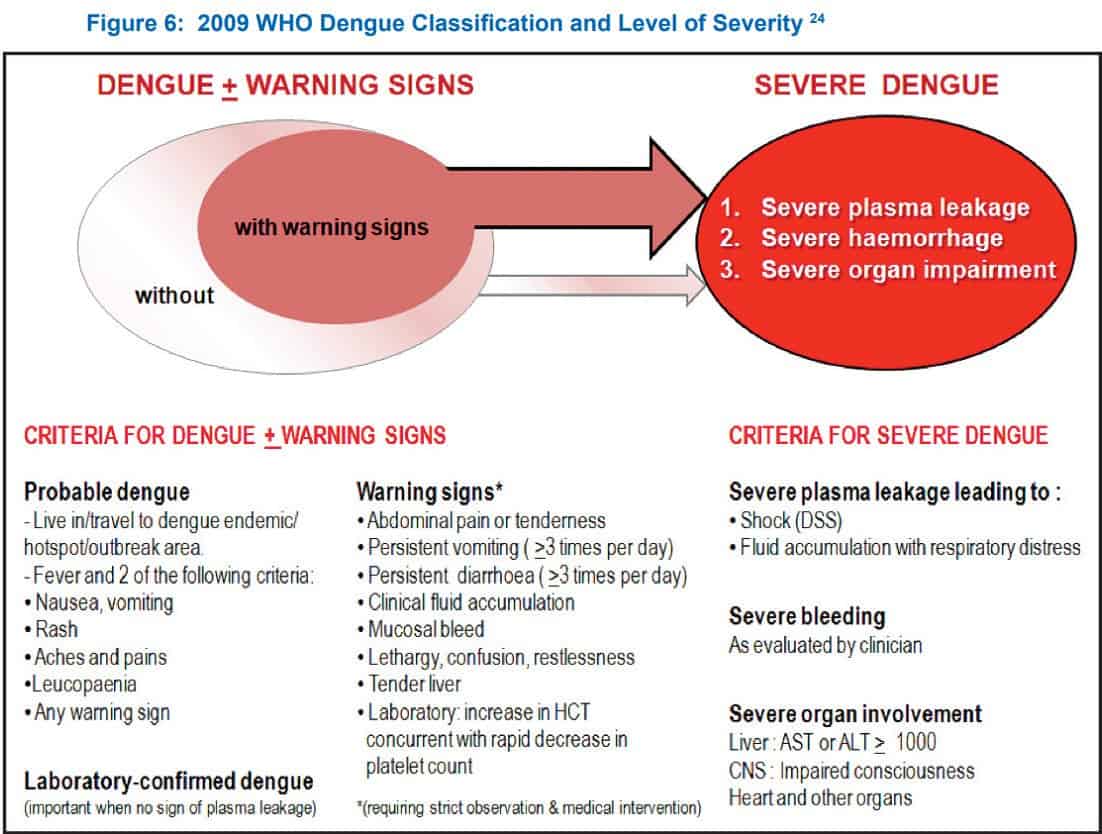
Abdominal pain, persistent vomiting and/or diarrhoea, restlessness, altered conscious level, clinical fluid accumulation, mucosal bleed or tender liver are the clinical warning signs of dengue infection with high possibility of complications.
Organ dysfunctions such as hepatitis, encephalitis and myocarditis usually but not exclusively occur during this phase. It is important to note that thrombocytopaenia and haemoconcentration are usually detectable in this phase.
Blood
– Hematocrit raised
– White cell count drop
– Coagulation profife deranged – clotting abnormalities,
– Transaminase – typically the level of (AST) > (ALT),
– Hypoproteinaemia and hypoalbuminaemia are usually observed.
iii. Recovery/Reabsorption Phase
After 24-48 hours of critical phase, usually plasma leakage stops followed by reabsorption of extravascular fluid. Patient’s general well being improves, appetite returns, gastrointestinal symptoms improve, haemodynamic status
stabilises and diuresis ensues. Some patient may have a classical rash of “isles of white in the sea of red” with generalised pruritus.
It is important to note that during this phase, HCT level stabilises and drops further due to haemodilution following reabsorption of extravascular fluid. The recovery of platelet count is typically preceded by recovery of white cell count (WCC).
In some instances, organ dysfunctions may worsen (hepatitis, encephalitis and intracranial bleed) as the patient enters reabsorption phase.
Pathophysiology Of Plasma Lakage In Severe Dengue
The primary pathophysiological abnormality seen in dengue infection is an acute increase in vascular permeability that leads to leakage of plasma into the extravascular compartment, resulting in haemoconcentration and hypovolaemia or shock.
Hypovolaemia leads to reflex tachycardia and generalised vasoconstriction due to increased sympathetic output.
Clinical manifestations of vasoconstriction:
- Skin – coolness, pallor and delayed capillary refill time
- CVS – raised diastolic blood pressure and a narrowing of pulse pressure
- Renal – reducing urine output
- GIT – persistent vomiting, persistent diarrhoea and abdominal pain
- CNS – lethargy, restlessness, apprehension, reduced level of consciousness
- Respiratory – tachypnoea (respiratory rate >20/min)
Inadequate perfusion of the tissue leads to increased anaerobic glycolysis and lactic acidosis. If the hypovolaemia is not corrected promptly, the patient will progress to a refractory shock state. By then, the tissue perfusion would not respond to vasopressor drugs, even if the blood pressure and intravascular volume were to be restored and cardiac output would remain depressed. The resultant lactic acidosis further depresses the myocardium and worsens the hypotension.
Prevention
Approach To Outpatient Evaluation Of Dengue Infection
History
- Date of onset of fever/illness
- Oral intake
- Assess for warning signs
- Change in mental state/seizure/dizziness
- Urine output (frequency, volume and time of last voiding)
- Other important relevant histories:
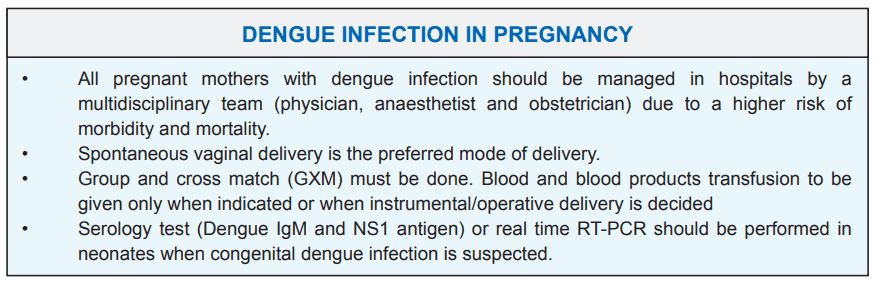
- Pregnancy
- Co-morbidities
Physical examination
i. Assess mental state and GCS score
ii. Assess hydration status
iii. Assess haemodynamic status
- CCTVR – Skin colour (C), CRT < 2 seconds (C), cold/warm extremities (T), pulse volume (V), rate (R)
- Blood pressure and pulse pressure (narrow?)
iv. Look out for tachypnoea/acidotic breathing/pleural effusion
v. Check for abdominal tenderness/tender liver/ascites
vi. Examine for bleeding manifestation
Investigation
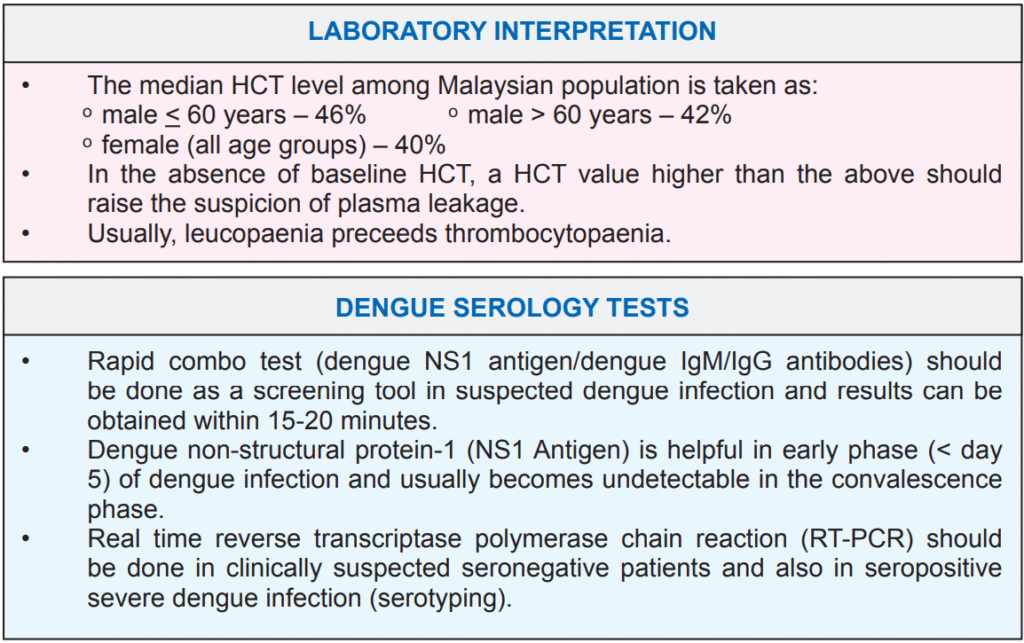
i. FBC and HCT
ii. Point of care test for dengue infection (RCT or NS1 antigen)
Diagnosis, disease staging and severity assessment
Based on evaluations in history, physical examination ± FBC, HCT and point of care test, the clinicians should be able to determine:
- Likelihood of dengue infection
- The phase of dengue infection (febrile/critical/recovery)
- Severity of the illness
Plan of management
- Dengue assessment checklist must be filled
- Notify the district health office followed by disease notification form
- If admission is indicated
- Stabilise the patient at primary care before transfer
- Communicate with the receiving hospital/Emergency Department (ED) before transfer
- At ED, dengue patients with deteriorating vital signs must be uptriaged accordingly
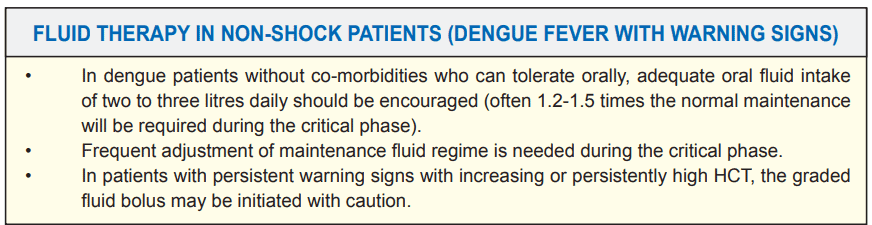
- Those requiring admission should be immediately started on an appropriate fluid therapy (oral or IV)
- Chest X-ray and ultrasound (where available) are required in patients suspected to have vascular leakage.
- If admission is not indicated
- Daily follow up is necessary until the patient remains afebrile for at least 24 – 48 hours
- Provide patient with Outpatient Dengue Monitoring Record and Home Care Advice Leaflet for Dengue Patients
Common Pitfalls In Fluid Therapy
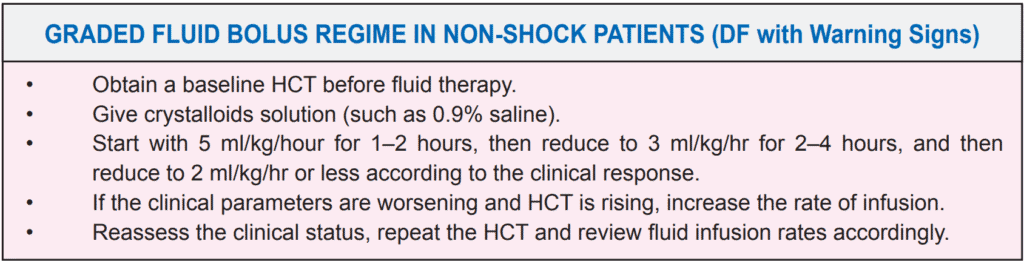
- Treating patients with unnecessary fluid boluses based on raised HCT or warning signs as the sole parameter without considering other clinical parameters.
- Excessive and prolonged fixed fluid regime in stable patients.
- Infrequent monitoring and adjustment of infusion rate.
- Continuation of intravenous fluid during the recovery phase.
- Excessive fluid therapy in patients with co-morbidities (such as heart disease and renal disease).
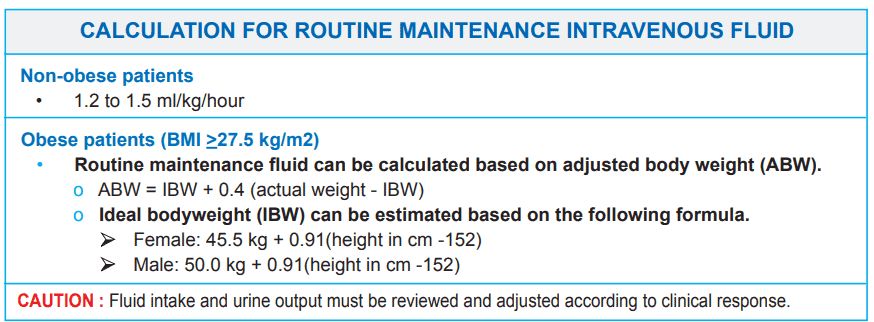
Dengue Fluid Calculator For Obese (BMI > 27.5)
Dengue Shock Syndrome (DSS)
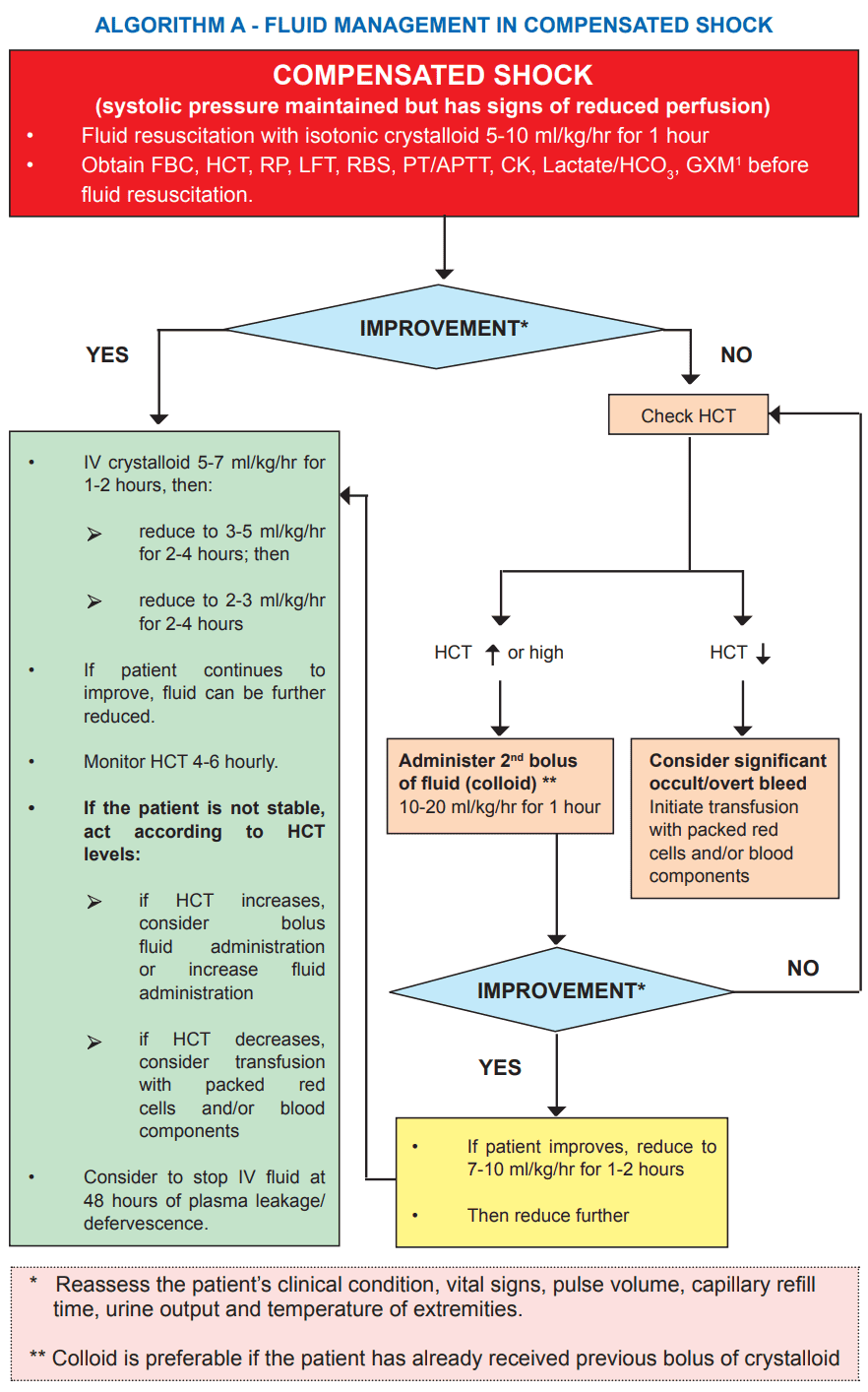
Dengue shock syndrome is a medical emergency. Recognition of shock in its early stage (compensated shock) and prompt fluid resuscitation will give a good clinical outcome. However, failure to recognise the phase of compensated shock will ultimately lead to decompensated (hypotensive) shock with a more complicated disease course and organ failures.
Pulse pressure of <20 mmHg and systolic pressure <90 mmHg are late signs of shock in adults
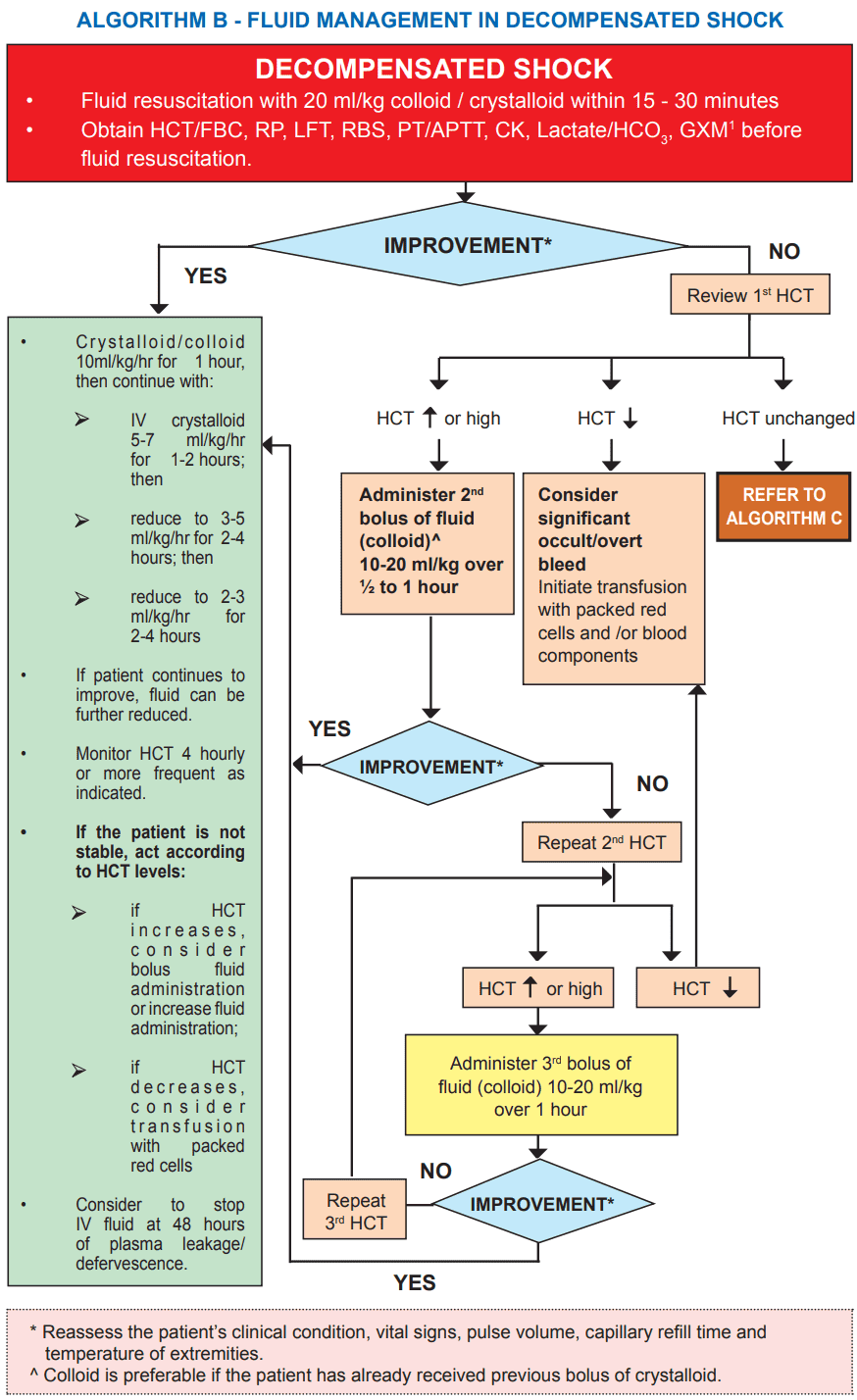
Non-responders to Initial Resuscitation (Refer to Algorithm A and B)
If the first two cycles of fluid resuscitation (about 40 ml/kg) fails to establish a stable haemodynamic state and HCT remains high, further bolus of colloids should be considered for the third cycle. (refer to Algorithm A and Algorithm B)
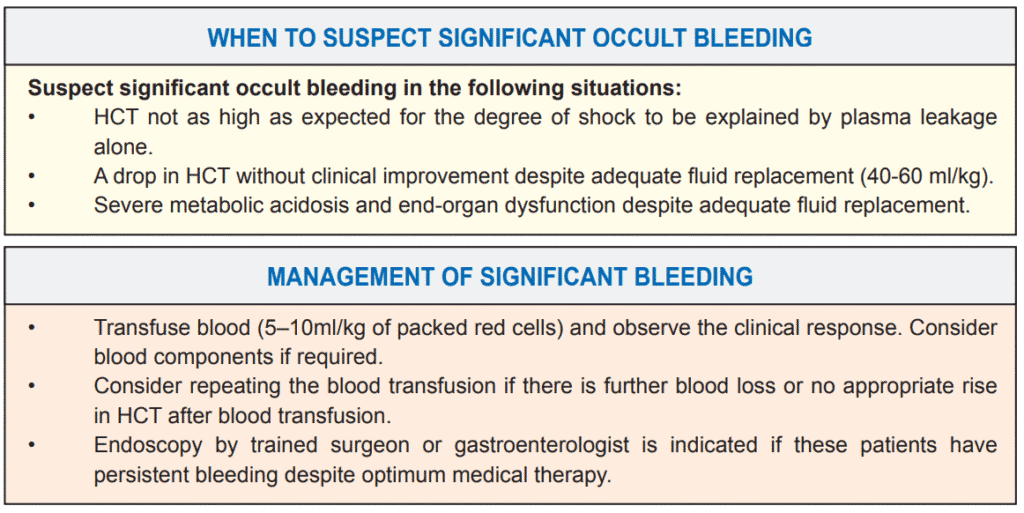
If the repeat HCT drops after two cycles of fluid resuscitation and the patient remains in shock, one should suspect significant bleed (often occult) for which blood ± blood products transfusion needs to be instituted promptly. (refer to Algorithm A and Algorithm B)
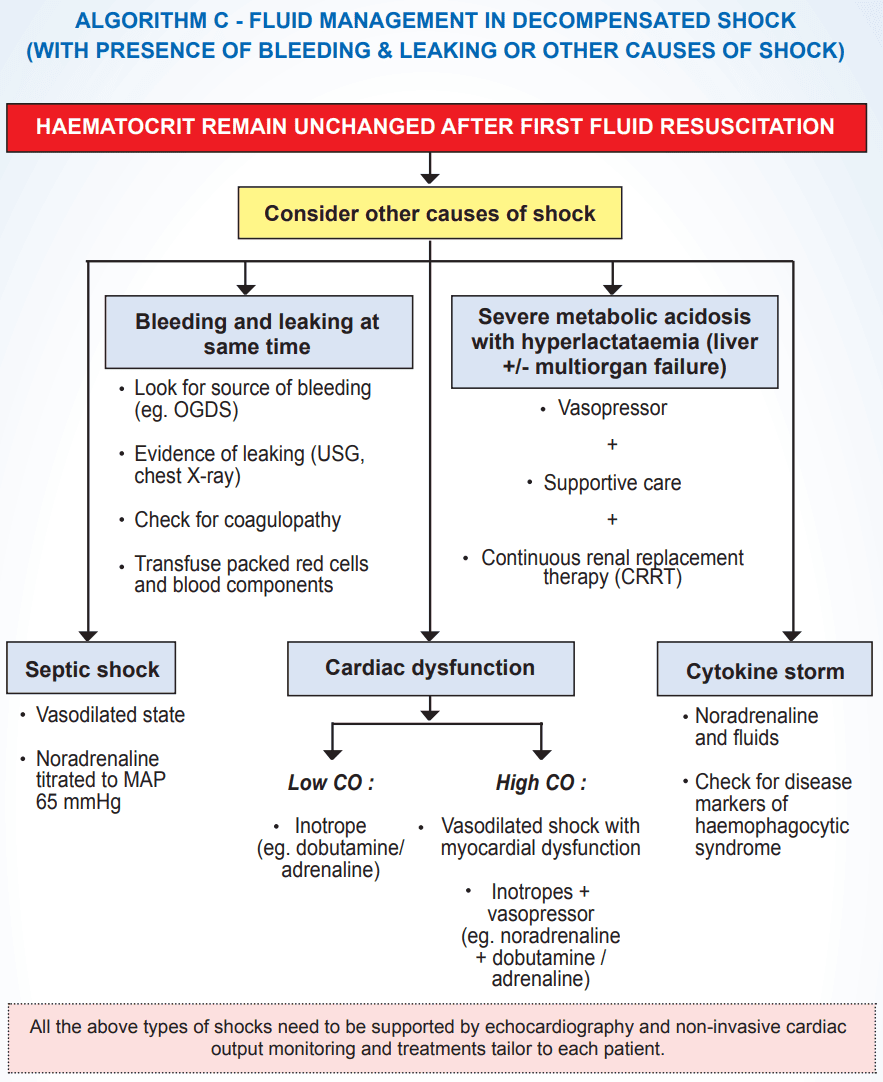
Other possible causes of persistent shock include: (refer to Algorithm C)
- sepsis
- cardiogenic shock (due to myocarditis, cardiomyopathy, RV/LV dysfunction, pericardial effusion or cardiac ischaemia),
- cytokine storm (a vasodilated state due to release of inflammatory mediators)
- liver failure with lactic acidosis.
Fluid therapy has to be judiciously controlled to avoid fluid overload which could result in massive pleural effusion, pulmonary oedema or ascites.